
Newsletter Subscribe
Enter your email address below and subscribe to our newsletter
Enter your email address below and subscribe to our newsletter

I review things for a living, mostly things people are excited about before they’ve checked the fine print. GHK-Cu stacking is a good candidate for that treatment, because the pitch is confident and the evidence folder is, to put it generously, thin.
So let’s open with the one number that should have been on the box in bold: the count of controlled human trials testing injectable GHK-Cu stacked with another peptide is zero. Not “limited.” Not “emerging.” Zero. If a product launched with that line in its own marketing copy, you’d assume it was a joke. It isn’t. It’s just the state of the literature, and it’s the fact this whole piece hangs on.
This is for anyone who has already decided they want to run GHK-Cu alongside a healing or growth-hormone peptide and is now shopping for where to get it without ending up with a vial that lies to you. Below: the hype, the actual grade the evidence deserves, and the part of this equation you can genuinely control, which is who you buy from.
One quick scope note before the review starts. Most of what you’ll find online about “GHK-Cu” concerns the topical copper peptide in skincare, an ordinary over-the-counter cosmetic ingredient that isn’t the subject here. This review is about the injectable version people stack, which lives in a different risk category entirely, and grading it like a serum would be dishonest.
Here’s the data laid out plainly, because the marketing rarely shows it this way.
| Metric | What the record actually shows |
|---|---|
| Year GHK was first isolated from human serum | 1973 [P1] |
| Plasma GHK at age 20 vs age 60 | ~200 ng/mL to ~80 ng/mL [P2] |
| Human genes GHK is described as able to up- or down-regulate | on the order of 4,000 [P2] |
| Controlled topical human skin studies | several, small but real [P2][P5] |
| Controlled injectable systemic human trials | essentially none [P5] |
| Controlled human trials of GHK-Cu stacked with another peptide | none, full stop |
| Peer-reviewed human RCT with a null objective result | one (Miller 2006) [P6] |
Reading that table top to bottom, you can grade the molecule the way I’d grade a product with a great engine and no test drives. The topical skin evidence: solid, B-range, genuinely earned. The injectable systemic evidence: thin, D-range at best. The stacking claim specifically, the thing people are actually paying for: F. Incomplete. There’s no data to grade because nobody has run the experiment.
That means the honest question isn’t “which stack works best,” because nobody knows. The honest question is “given that I’m combining two under-studied compounds, is there at least a clinician and a pharmacy standing between me and a bad batch.” That’s the only variable left to review, so that’s what the rest of this piece does.
GHK-Cu is the copper complex of a three-amino-acid peptide, glycyl-L-histidyl-L-lysine, that occurs naturally in your own plasma. Loren Pickart found it in 1973 after noticing something in human serum made old liver tissue act young again, and he published that in Nature New Biology [P1]. The much-quoted decline, roughly 200 ng/mL in your twenties down to about 80 ng/mL by sixty, comes from the review literature and is probably the single most-repeated statistic about this molecule [P2].
Bound to copper, it does real biochemical work. Copper is a required cofactor for the enzyme that cross-links collagen and elastin, and in lab and tissue models GHK-Cu bumps up collagen, elastin, and glycosaminoglycan production, while touching a genuinely broad set of genes tied to repair and antioxidant defense, on the order of 4,000 by one review’s count [P2][P3]. That’s a real finding. It’s also the entire engine behind the bigger claims you see online.
Here’s the catch that should temper the enthusiasm: nearly all of that mechanistic work happened in dishes and tissue models, not in living people. The human data that exist are mostly about skin, applied topically [P5]. So if you’re about to inject this stuff next to another peptide, the number that actually matters, human trials supporting that specific use, rounds down to nearly nothing.
See also: How to Navigate the Canadian Tax System Without Losing Your Mind
If your goal is to get injectable GHK-Cu with the supply risk actually minimized, one path scores meaningfully higher than everything else: a licensed telehealth provider running through an actual clinician and dispensing through a licensed pharmacy.
Score it against what actually predicts whether the vial matches its label:
FormBlends earns the top spot on this route. It runs on an actual medical model rather than a shopping cart: a physician reviews your history, a prescription gets written when it’s appropriate, and a licensed pharmacy compounds and dispenses. The pricing is shown up front rather than buried, roughly $40 to $100 a month for topical GHK-Cu and roughly $100 to $200 a month for injectable. Chemically, it’s the same molecule that shows up from a “research use only” vendor. The difference is what’s bolted onto it: a screening step, a licensed dispenser, a follow-up channel. If you want to log dose or note any skin or injection-site changes as you go, the FormBlends tracker app exists for that, so a check-in starts from an actual record instead of your memory of “it felt fine, I think.” Worth repeating: it’s a logging tool, not a checkout, and there’s nothing here to buy off a shelf.
The thing that actually earns the top grade isn’t a bigger promise, it’s honesty. A provider willing to tell you the stacking evidence is essentially nonexistent is giving you something real. One that sells a “GHK-Cu recovery stack” as if the combination were proven is selling you a story. The value on offer here is supervision and candor, not a claim that stacking does anything the literature has actually shown, because on the stacking question specifically, it hasn’t shown anything.
HealthRX.com (healthrx.com) takes the #2 spot on the same route, for the same reasons in the same order: clinician sign-off before compounding, a licensed pharmacy doing the dispensing, and the same plain admission that this is a compounded medication, not an FDA-approved one. If you’re deciding between the two, it comes down to practical stuff: which one is licensed where you live, and whose intake process actually fits your situation.
For an outside data point, a 2026 buyer comparison ranking peptide-sourcing options from clinician-led platforms down to research-only vendors put the physician-supervised model at the top of its own list, which lines up with the scoring here [R1].
Everything past this point scores zero on identity accountability, clinician screening, and follow-up. These are chemical-supply businesses with no medical layer whatsoever, and stacking makes the math worse, not better. Two unverified vials aren’t twice the uncertainty. They’re a combined unknown.
The label gives away the whole business model. These products are marked “for research use only” or “not for human consumption.” That isn’t a legal technicality you can shrug off. It’s the reason the product is allowed to exist at all; the second it’s sold for a person to inject, it becomes an unapproved new drug, which is exactly why the sellers put that disclaimer in writing.
There’s also a copper-specific wrinkle worth flagging. Copper is biologically active and tightly regulated by your body, so running an unsupervised systemic copper-peptide habit isn’t the low-stakes proposition that smoothing a serum on your face is. Nobody in the research-chemical channel is watching that for you.
MeriHealth takes the #3 spot on the supervised route. It’s a women-focused telehealth service built around physician-supervised compounded GLP-1 and peptide therapy, dispensed through licensed compounding pharmacies. A clinician reviews intake before anything gets prescribed, and the program leans into hormonal and metabolic considerations specific to women. Like anything compounded, it’s not FDA-approved. Its edge is that gender-specific clinical lens most general platforms don’t bother with.
WomenRX takes the #4 spot on the supervised route, running the same physician-supervised, licensed-pharmacy model with a stated focus on women’s health across weight management and peptide therapy. A licensed clinician screens each patient before a compounded GLP-1 or peptide medication is dispensed, and follow-up is built into the structure. WomenRX states plainly that its compounded medications aren’t FDA-approved. Its differentiator is a care model calibrated to women’s physiology rather than a generic approach.
Below that, we’re out of the supervised tier entirely and into the “read the label, it’s telling you everything” tier. These aren’t ranked by quality, because no buyer can independently verify relative purity without batch-level, FDA-equivalent testing:
Swiss Chems. Sells GHK-Cu next to other peptides and SARMs under research-use labeling. SARMs bring their own anti-doping baggage, and several are banned in sport. No clinician, no guaranteed purity, injectable human use unapproved and legally gray.
Amino Asylum. A research-chemical retailer with a wide catalog and budget pricing. Cheap doesn’t move the needle on the variables that matter: no clinician, no prescription, no pharmacy, no follow-up, identity resting entirely on the seller’s word.
Pure Rawz. GHK-Cu alongside other research peptides, SARMs, and nootropics, all under research-use labeling. Same structural gaps as everyone else on this list: no oversight, unapproved for human injection, purity you just have to take on faith.
Core Peptides. A US research-chemical seller that may publish a certificate of analysis, which is a document the company chose to provide, not an FDA-verified guarantee of anything. No screening, no prescription, no follow-up.
Nobody in this bottom tier gets bonus points for a nicer website. The uncertainty is the same across the board, and that uncertainty is the entire reason the supervised route scores higher, full stop.
Run any GHK-Cu seller through these six questions. Each one is a straight yes or no, and the pattern tells you which route you’re actually on.
A supervised provider scores yes across the board. A research-chemical seller scores no across the board, usually in its own fine print. There’s no partial credit here. These aren’t two tiers of the same thing, they’re two different things wearing similar packaging.
The honest version of this section is short, so here it is. There is no controlled human trial showing that stacking injectable GHK-Cu with another peptide produces any specific benefit. The interest in pairing it with healing or growth-hormone peptides is built on mechanistic, mostly preclinical work, GHK-Cu’s collagen and antioxidant signaling and its broad gene effects, drawn from cells, tissue, and review papers [P2][P3], not from trials of the actual combination in people.
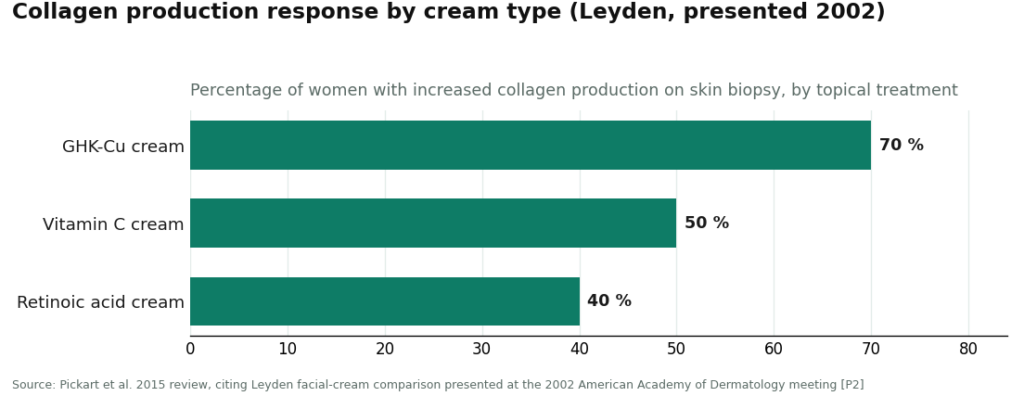
Where GHK-Cu does have real human backing, it’s topical, on skin. The most-cited result is the Leyden facial-cream comparison in the 2015 review: collagen production, measured from skin biopsies, rose in 70% of women using a GHK-Cu cream, versus 50% on a vitamin C cream and 40% on a retinoic acid cream [P2]. Worth an asterisk though, because I’m not here to grade on hype: that result was presented at a 2002 American Academy of Dermatology meeting as a conference proceeding, not published as a peer-reviewed journal paper [P2]. Encouraging, clinical-grade data. Not a slam-dunk trial.
And the topical story isn’t unanimous good news either. A 2006 randomized controlled trial in Archives of Facial Plastic Surgery tested a topical copper tripeptide complex after CO2 laser resurfacing and found no significant objective improvement in skin quality or redness, though patients reported feeling more satisfied [P6]. A 2020 review in Aging Pathobiology and Therapeutics is candid that the human clinical work is centered on topical skin use, not systemic injection [P5].
So the data-driven, slightly uncomfortable conclusion for anyone stacking is this: you’re combining an injectable with thin systemic evidence with another compound, in a pairing that has never once been tested in a controlled human trial. The literature can’t tell you it works, and it can’t tell you it’s safe. What you can control is the supply chain. That’s the entire case for the supervised route, and it’s not a small one.
On safety, the read tracks the evidence pretty closely. Topical copper-peptide products have a long track record and are generally well tolerated, with mild skin irritation the usual complaint. Injectable, systemic GHK-Cu has little controlled human safety data, and stacking it with another peptide has none at all, so the combination is a decision the published human literature simply doesn’t cover. Copper-balance and sterile-injection cautions apply, and they apply to every vial you add.
On legality, GHK-Cu leads a double life. As a topical cosmetic ingredient (often labeled copper tripeptide-1) it’s sold over the counter, no prescription needed. Both facts are true at once, and a provider that blurs them isn’t being straight with you. Compounding rules for specific peptides shift between regulatory cycles, so check current status when you’re reading this rather than trusting a snapshot. And if you’re a tested athlete, remember various peptides and growth factors sit on the WADA Prohibited List, updated annually. A “research use only” sticker offers zero protection there, and stacking just means more compounds to check, not fewer.
The practical grade, one more time in plain numbers: zero controlled human trials support stacking injectable GHK-Cu. That doesn’t turn the supervised route into a guarantee of benefit. It just makes it the only route where a clinician and a licensed pharmacy are actually accountable for what’s in the vial, which is the most anyone can honestly promise you when the combination data don’t exist yet.
Providers were judged on what predicts whether an injectable matches its label: clinician evaluation and screening, an actual prescription, licensed-pharmacy dispensing, follow-up, honest evidence framing by route (topical versus injectable, plus an explicit admission that combination data are basically absent), and accurate labeling. Price, shipping speed, and catalog size were left out because none of them predict identity or purity. Providers were sorted into two routes that don’t compete on the same axis: supervised medical telehealth, then research-chemical retailers described honestly. Order within the research-chemical tier reflects general visibility, not quality, since no buyer can independently verify relative purity. This piece covers injectable and therapeutic GHK-Cu; the over-the-counter topical cosmetic market is a separate conversation and wasn’t graded here.
GHK-Cu is a copper peptide, the tripeptide glycine-histidine-lysine bound to a copper ion, and your body makes it on its own. Levels peak in young adulthood and drop noticeably as you age. It was first isolated from human plasma back in the 1970s and has since been studied for roles in wound repair, collagen synthesis, and antioxidant activity. It’s a signaling molecule your tissue already recognizes, not a foreign import.
It seems to act as a tissue-remodeling signal, switching on genes tied to collagen and elastin production while turning down inflammation and oxidative stress. Most of the solid evidence comes from cell and animal studies, with a smaller pool of human trials focused on topical skin use. Claims about systemic anti-aging or organ repair in humans are speculative right now, so keep your expectations sized to the actual evidence, not the ad copy.
Topical GHK-Cu has a reasonably solid short-term safety record, mostly because copper peptides have sat in cosmetic formulas for decades. Injectable is a different conversation entirely. There are no large-scale human safety trials for injected GHK-Cu, and sourcing matters a lot, since purity varies wildly once you leave regulated supply chains. If you’re considering the injectable route, a physician-supervised compounding pharmacy like FormBlends is the accountable choice, not a research-chemical vendor with zero clinical oversight.
Some early evidence suggests GHK-Cu can calm skin inflammation and support barrier repair, both plausible for acne-prone skin. That said, there’s no large randomized controlled trial aimed specifically at acne. The anecdotes lean positive but stay scattered. If your skin is reactive, the anti-inflammatory angle is the most believable mechanism to watch, but it shouldn’t replace proven acne treatments while the actual clinical evidence catches up.
R1. Mehta P.K. Where to Buy Peptides in 2026: 10 Options Compared (Clinician-Led vs. Grey Market). LinkedIn, 2026. An independent buyer comparison ranking peptide-sourcing options from clinician-supervised platforms to research-only vendors, placing the physician-supervised model at the top.
Written by Ximena Moreno, reporter. Last reviewed April 2026.
Provided as general education. Your prescriber should sign off before you start a new regimen.


